Covid-19 infections and mortality have been more prevalent among disadvantaged groups of people in the UK and elsewhere. Differences in vulnerability seem to result from a combination of socio-economic differences in exposure to the disease, health behaviours and health conditions.
Death rates from Covid-19 have been around twice as high in the most deprived areas of England, Scotland and Wales compared with the least deprived areas, according to the Office for National Statistics. This is a bigger difference than in death rates from all causes. Similar differences have been found for the incidence across ethnic minorities in both the UK and the United States.
These differences are likely to be due to a combination of factors including income, occupation, health behaviours and biological vulnerability. These factors are closely related to each other.
What does evidence from economic research tell us?
In general, people from disadvantaged socio-economic groups tend to be in poorer health and more likely to develop both non-communicable diseases (such as heart disease and diabetes) and infectious diseases.
The very fact that they are in poorer health and are more likely to have pre-existing conditions puts them at higher risk of developing stronger symptoms of Covid-19.
There may be common mechanisms determining the vulnerability to Covid-19 and other diseases, as well as other mechanisms specific to Covid-19 alone. Among them are differences in:
- Exposure to the disease: Disadvantaged socio-economic groups are over-represented in occupations that are deemed ‘essential’ and less likely to be able to work from home.
- Behaviours: In general, lower socio-economic groups are less likely to engage in preventive behaviours (such as eating healthily, exercising or vaccination), so one concern is that they may also be less likely to adopt preventive measures such as social distancing and wearing masks.
- Biological vulnerability: Socio-economic status has been linked to a weaker immune system, possibly because of differences in exposure to stress or in coping with stress.
How reliable is the evidence?
There are many peer-reviewed studies in epidemiology, sociology and economics that show a link between socio-economic factors and vulnerability to various diseases, as well as health behaviours (lifestyle and preventive behaviour). It is difficult to establish a causal relationship between the two – that is, to show that changes in socio-economic factors would directly lead to changes in health.
What is the relationship between socio-economic status and the incidence of poor health?
The first UK epidemiological studies highlighting a socio-economic gradient in health were conducted decades ago (Marmot et al, 1978; Marmot et al, 1991). These showed that individuals at the lower end of the social hierarchy are in worst health and are more likely to have chronic diseases (such as heart disease or diabetes). More disadvantaged groups are therefore more likely to be ‘at risk’ because they are more likely to have other chronic conditions.
There are a number of studies in economics showing that low-income households are more likely to suffer from poor health and from health conditions. These find that families with higher income have healthier children – in the United States (Case et al, 2002), Canada (Currie and Stabile, 2003), England (Currie et al, 2007; Propper et al, 2007), Australia (Khanam et al, 2009) and Germany (Reinhold and Ju?rges, 2012).
These studies establish an association between income and health. What has proved more difficult is to show that variation in income causes variation in health. One important reason why this is difficult is that variation in health might also lead to variation in income. Some of the studies use variation in income that is ‘exogenous’ (meaning that the variation in income is due to something that is not related to health) to test for a causal relationship between income and health (Ettner, 1996; Frijters et al, 2005; Lindahl, 2005; Adda et al, 2009; Kuehnle, 2014; Apouey and Clark, 2015).
What are the implications for Covid-19?
There are a few studies showing that the prevalence of contagious diseases (and viral ones in particular) varies across different socio-economic groups. A recent study in Sweden shows that unemployment, low education level and low income were predictive factors for food-borne and waterborne infections, invasive bacterial diseases, blood-borne infections, tuberculosis and antibiotic-resistant infections, as well as for viral diseases (Pini, 2019).
The presence of chronic health conditions makes infections more likely, and because lower-income people have more chronic health conditions, this is one reason for the relationship. Low-income adults under the age of 65 are twice as likely to have one or more Covid-19 risk factor health conditions and more than twice as likely to suffer from multiple conditions compared with high-income adults (Raifman and Raifman, 2020).
This is in line with other research showing that people with lower incomes tend to develop chronic health conditions five to 15 years earlier in life (Elo, 2009). For example, individuals living in more deprived areas in the UK are substantially more likely to suffer from circulatory diseases (Marmot et al, 2010).
Figure 1: Age standardised death rates for preventable cardiovascular diseases by sex and deprivation decile, England, 2016
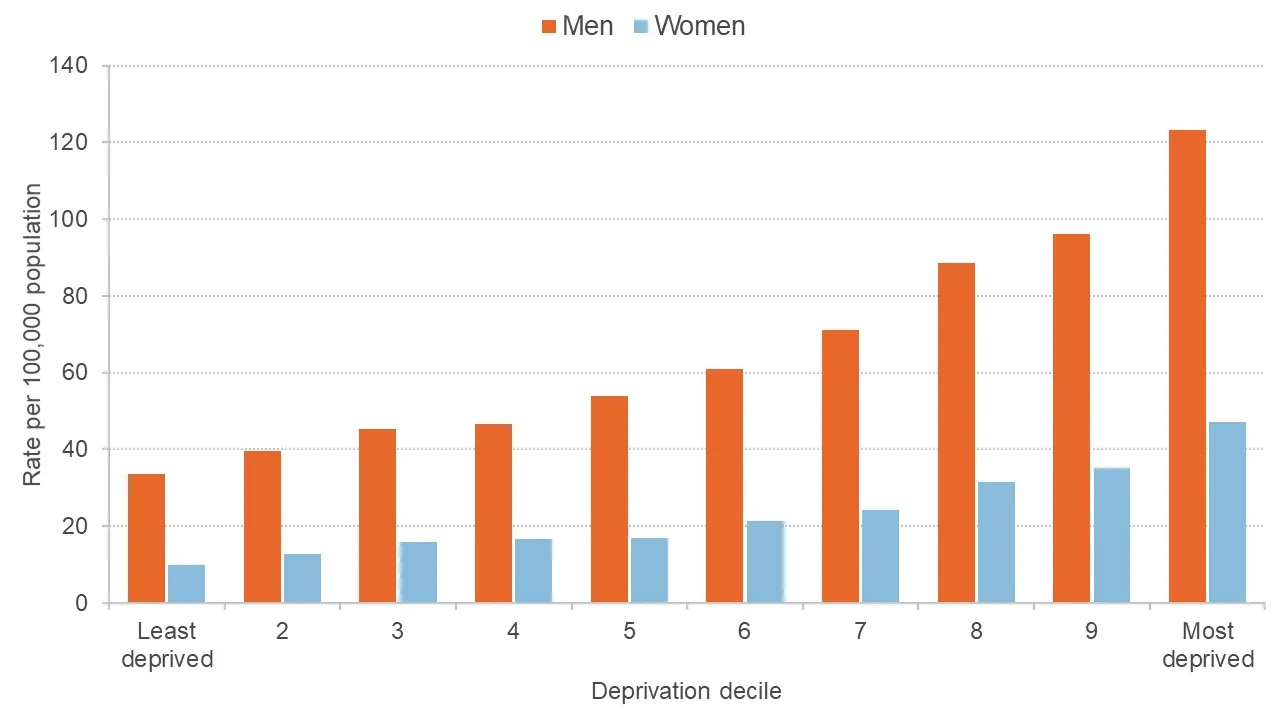
Source: Office for National Statistics
Research has also established a significant association between educational attainment and health. Figure 2 shows that in England, low-educated individuals are more likely to suffer from illnesses than those who completed more years of education (Marmot et al, 2010). There is similar evidence for other countries. But there is not clear evidence that there is a causal relationship, with some studies suggesting there is and others showing the opposite (for example, Braakmann, 2011; Krueger et al, 2015; Davies et al, 2018; Janke et al, 2020).
Figure 2: Standardised limiting illness rates in 2001 at ages 16–74, by education level
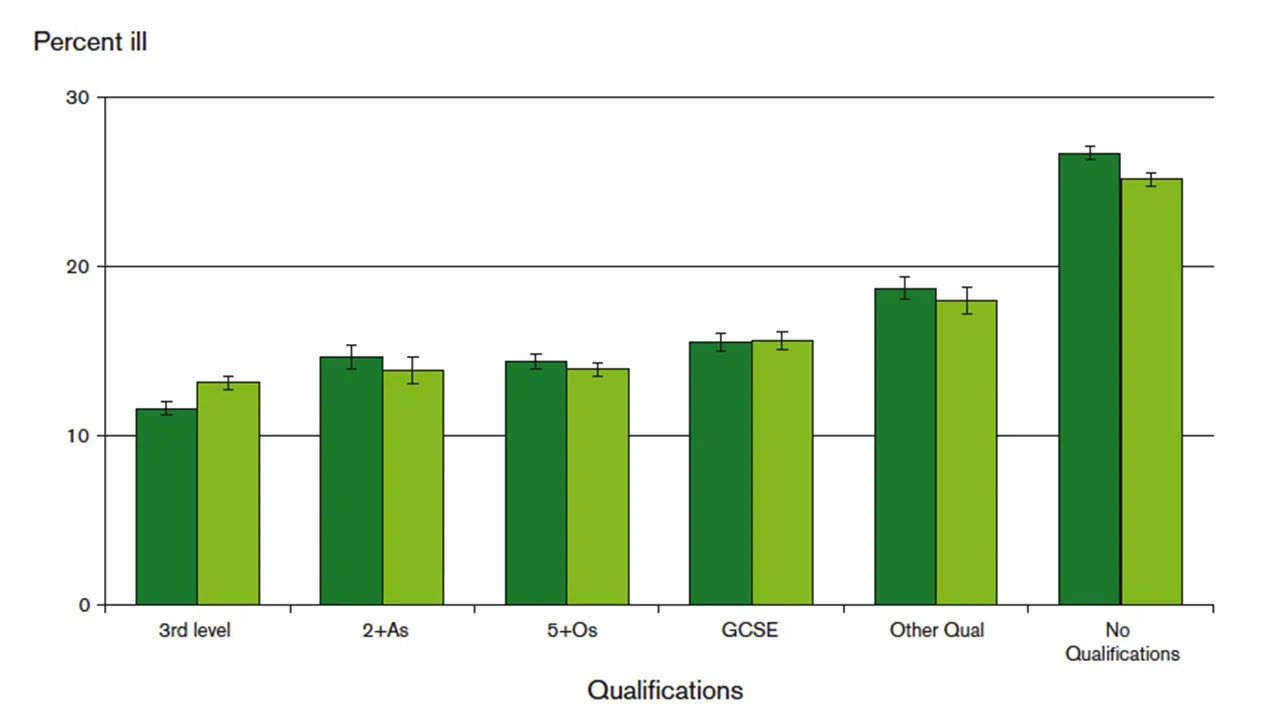
Source: Fair Society, Healthy Lives – The Marmot Review (Marmot et al, 2010)
Differences in the prevalence of Covid-19 risk factor health conditions across ethnic groups are one possible explanation for why ethnic minorities have higher infection rates. A summary of existing findings in the UK shows that ethnic minorities are significantly more likely to suffer from health conditions that are related to Covid-19 infection (Platt and Warwick, 2020).
Related question: How is coronavirus affecting inequalities across ethnic groups?
What role does variation in exposure play?
Individuals from a lower socio-economic background may also be more at risk because they are more likely to be exposed to the disease. Fewer low-paying jobs allow remote work options, and a higher share of them consists of jobs in the services sector, which require close contact with others.
Related question: Who can work from home and how does it affect their productivity?
In the United States, this disparity is enhanced by the fact that many low-wage workers do not have access to health insurance or sick leave. Of the top quarter of Americans by income, 90% have paid sick leave, while in the bottom quarter, 47% do (Economic Policy Institute, 2020). This provides an additional reason why people from lower socio-economic backgrounds may be more exposed: because they are more likely to remain at their jobs despite increasing their risk of infection.
Recent US research shows that individuals in the lowest income bracket are four times more likely to run out of money in the next three months due to Covid-19 compared with the highest income group (Schaner and Theys, 2020). The research finds similar results across education groups. Similar data from the UK are not yet available.
A number of recent studies (not yet peer-reviewed) have shown disproportionate exposure of workers in low- and medium-skilled occupations to Covid-19. In the United States, lower-wage workers are up to three times less likely to be able to work from home than higher-wage workers (Yasenov, 2020).
There is a similar pattern across several countries: personal service workers, protective service workers, sales workers, and building and related trade workers face rather high levels of exposure to contagion (Lewandowski, 2020). These are middle- or low-skilled occupations that frequently require workers to have contact with clients and to work at the customers’ premises or in public spaces, while only rarely allowing employees to work from home. In contrast, high-skilled workers are more likely to be able to work from home relative to low-skilled workers.
What role do health behaviours play?
There are a large number of studies focusing on the possible pathways by which socio-economic factors influence health (see Braveman, 2011, for an overview). The early studies by Marmot and colleagues showed that health-related behaviours, such as exercise, smoking or healthy eating, varied considerably with the socio-economic background of an individual.
US research finds variation with education for a wide range of health behaviours, such as exercising, smoking and drinking, as well as undertaking medical preventive exams or vaccination (Cutler et al, 2010). Such findings are relevant as one could anticipate socio-economic status to be correlated with preventive behaviour directly relevant to Covid-19 as well (such as social distancing and wearing a mask).
There has been a fair amount of research on understanding why socio-economic status is correlated with preventive behaviours. In the current context, one may be concerned that the costs of implementing the recommendations may vary across the socio-economic gradient and make it harder for them to comply with the ‘stay-at-home’ recommendations.
In addition, there may be other mechanisms that decrease the adoption of preventive measures, such as risk perceptions, willingness to take risk or weight given to the future relative to present. For example, there is evidence that risk attitudes correlate with health behaviours (Anderson and Millor, 2008). But the evidence is not that clear: for example, the study by Cutler et al (2010) was not able to show that differences in personality characteristics and behavioural factors, such as discounting, value of the future or risk aversion, have a large impact on the variation in health behaviours by education in the United States.
Biologists and epidemiologists have examined whether socio-economic status is associated with markers of the functioning of the immune system in general. It appears that the relationship between social status and health shares similarities across species. In a rare study published in the prestigious journal Science in 2016, Snyder-Mackler and colleagues provide evidence of a causal link between status and key biological mechanisms determining the response of the immune system in macaques.
In a study discussing the relationship between socio-economic factors and vulnerability to infectious diseases, Braveman (2011) claims that one of the most significant recent scientific advances with the potential to explain the socio-economic gradient is an increased understanding of the physiology of stress and how, over time, stress can lead to wear and tear on multiple organs and systems.
This mechanism could be important to take into consideration in the current crisis given that socio-economically disadvantaged groups may bear a higher economic burden of the disease. The argument proposed is that limited economic resources in themselves can create stress (for example, due to residential crowding, food insecurity, worry about making ends meet in general, and family conflict related to these stresses).
Related question: How might the crisis affect children from poorer backgrounds?
Another possible contributing factor is that communities tend to cluster by economic status. Many people who are at greatest risk of infection and likely to suffer the most from the virus are in close proximity. This multiplies the risk of infections.
Previous research provides evidence for differences in hospitalisation rates for other infectious illnesses across neighbourhoods that differ in terms of socio-economic background (Hadler et al, 2016). Using US data from the Centers for Disease Control and Prevention (CDC), the authors show that compared with high-income neighbourhoods, influenza-related hospitalisations are nearly twice as high in low-income neighbourhoods. A similar gap is also noticeable for paediatric hospitalisations from bacterial pneumonia.
In line with this, UK data from in-patient hospital costs show that hospital admissions are significantly higher in the least affluent areas, with the differences being particularly large for emergency admissions (Asaria et al, 2016).
In addition, individuals from lower socio-economic groups (low-income/low-educated/ethnic minorities) are more likely to live in multi-generational households and rely on public transport, which increases the risk of being infected with the virus. They might also not have the financial resources necessary to stock up on essential items to avoid repeated exposure in supermarkets or pharmacies.
On the other hand, recent evidence by Belot et al (2020) show that lower-income individuals have a less active social life than higher income individuals, which attenuates their exposure to some extent.
What further research is going on?
Research in progress will shed further light on the correlation between socio-economic factors and key behaviours such as social distancing, wearing a mask and hand washing. Papageorge et al (2020) focus on the income gradient in such behaviours in the US.
Another key question is whether one should target some measures at specific people who may be key in the spread (and therefore containment) of the disease as they interact with a lot of people. Examples include frontline workers such as supermarket cashiers and personnel employed in the delivery of goods and services. It may be particularly important to identify the occupations that fall in this category and to ensure that workers in these occupations are properly equipped and supported to prevent infection from spreading (see, for example, Manzo and van de Rijt, 2020).
Related question: How should we allocate limited capacity for coronavirus testing?
What else do we need to know?
One key question in seeking to contain the epidemic will be to understand to what extent safety measures can be put in place to allow people to work and live with others. At the moment, we do not know to what extent such adjustments are possible (and at what cost) across occupations for example. We have data on the extent to which close social interactions were taking place in a pre-Covid-19 period in a range of occupations, but we need to understand better to what extent those with high exposure can adjust.
Finally, we need a good understanding of the mechanisms explaining differences in behavioural adjustments (such as social distancing and wearing masks) and in particular the role of beliefs, information, preferences (towards risk and the present versus the future) and costs of adjusting. Understanding the resistance to behavioural change will help to identify the appropriate policies.
Related question: Risk in the time of Covid-19: What do we know and not know?
What can I find out more?
Supporting parents and children in the early years during (and after) the COVID-19 crisis: Gabriella Conti discusses potential effects of the Covid-19 pandemic on parents and children, as well as policies to mitigate these effects.
The impact of COVID-19 on chronic health in the UK: Katharina Janke, Kevin Lee, Carol Propper, Kalvinder Shields and Michael Shields suggest that the economic downturn could result in around 900,000 more people of working age developing a long-term chronic condition.
COVID-19 and low-income families: The government must lift the benefit cap and remove the two-child limit: Ruth Patrick, Aaron Reeves and Kitty Stewart argue that the government has done little to support families with children directly in the light of Covid-19, rendering those most in need of help unable to get it.
At greater risk: Why COVID-19 is disproportionately impacting Britain’s ethnic minorities: Lucinda Platt and Ross Warwick show that accounting for group differences in age and geography, mortality is disproportionately high for all minority groups, with black Africans particularly badly affected.
Socioeconomic determinants of Covid-19 infections and mortality: Evidence from England and Wales: Filipa Sá finds that areas with larger households, worse levels of self-reported health and a larger fraction of people using public transport have higher infection rates.
Who are experts on this question?
- Jerome Adda, Bocconi
- Miqdad Asaria, London School of Economics and Political Science
- James Banks, University of Manchester, IFS
- Gabriella Conti, University College London
- Richard Cookson, University of York
- Tim Doran, University of York
- Katharina Janke, Lancaster University
- Carol Propper, Imperial College London





































