India’s comparatively low mortality rate among people with Covid-19 has surprised experts. Some have attributed this to the country’s stringent lockdown and testing strategies, but questions are being raised about the reliability of the data and the accuracy of its interpretation.
India recently surpassed Brazil to become the second-worst country to be affected by the coronavirus pandemic. With a population of over 1.4 billion and over 90,000 new cases every day, India has the highest infection rates in the world (Financial Times, 2020). At the same time, India has maintained one of the lowest rates of fatality from Covid-19 cases: 1.7% as of 7 September 2020 compared with a world average of 4.2% (Economic Times, 2020).
The relatively low number of deaths attributed to Covid-19 has been used by the country’s authorities as proof that India is coping effectively with the pandemic. Efforts by the government, such as the ‘world’s most draconian lockdown’ (Biswas, 2020) and the focused and coordinated efforts to ‘test, track and treat’, have been cited as contributing towards the low fatality rate (The Hindu, 2020).
But with new research indicating that other factors could be linked to the low mortality rate, it is uncertain whether India’s Covid-19 case fatality rate (CFR) is actually an underestimation and whether it is a consequence of the country’s lockdown and other restrictive measures.
Clarity on this debate is crucial as the low CFR should not be interpreted in a way that leads the public to underestimate the threat from the virus or officials to relax restrictions prematurely. This is particularly significant as India has started to open up its economy despite infection rates rising steadily.
What do we know?
As the number of cases started to rise exponentially across major cities in India, media reports emerged about ‘the Indian Exception’, referring to the mystery of the country’s low numbers of Covid-19-related deaths (BBC, 2020). With the world average CFR at 4.2%, India has consistently maintained a low death rate since the virus first appeared in the country. There are four factors that could explain this:
- The effectiveness of restrictive measures imposed by the Indian government.
- India’s relatively younger population.
- The under-reporting of deaths.
- The interpretation of CFR.
Was India’s response to Covid-19 effective?
Many physicians and public health professionals have said that India’s stringent nationwide lockdown, which lasted for over a month, could have been instrumental in keeping infection and death rates low. But analyses following lockdown have suggested otherwise, as the policy has been described as a failure by many.
The Indian government announced the ‘world’s strictest’ lockdown in March when approximately 360 cases were reported across the country (Kumar, 2020). The public were given just a few hours of notice to prepare for lockdown, which resulted in several unforeseen and extreme consequences, particularly the internal migrant crisis. Thousands of people fled the cities on foot with scarce resources, and several died on their way from fatigue and starvation. Those migrants who finally made it home were in some instances refused entry due to fear of transmission (Patel, 2020).
Experts have criticised the use of Western strategies of lockdown for a country like India – and the lack of realistic planning is further evidenced by the migrant crisis (Bhattacharyya, 2020). As explained by Kaushik Basu, former chief economist at the World Bank, India’s lockdown failed because it did exactly what the policy should not do: it led to an unprecedented and uncontrollable mass movement of people all over the country, desperately trying to reach home as they had no other choice (Biswas, 2020).
The pandemic and lockdown greatly disrupted and weakened the country’s already failing economy and soon, the government began easing its restrictions in phases to boost economic activity despite the sharp rise in cases (BBC, 2020). The ensuing return of migrants and other social and economic activities resuming have inevitably caused a surge in new cases.
Figure 1: Covid-19 cases and strategies adopted by the government in the days leading up to lockdown
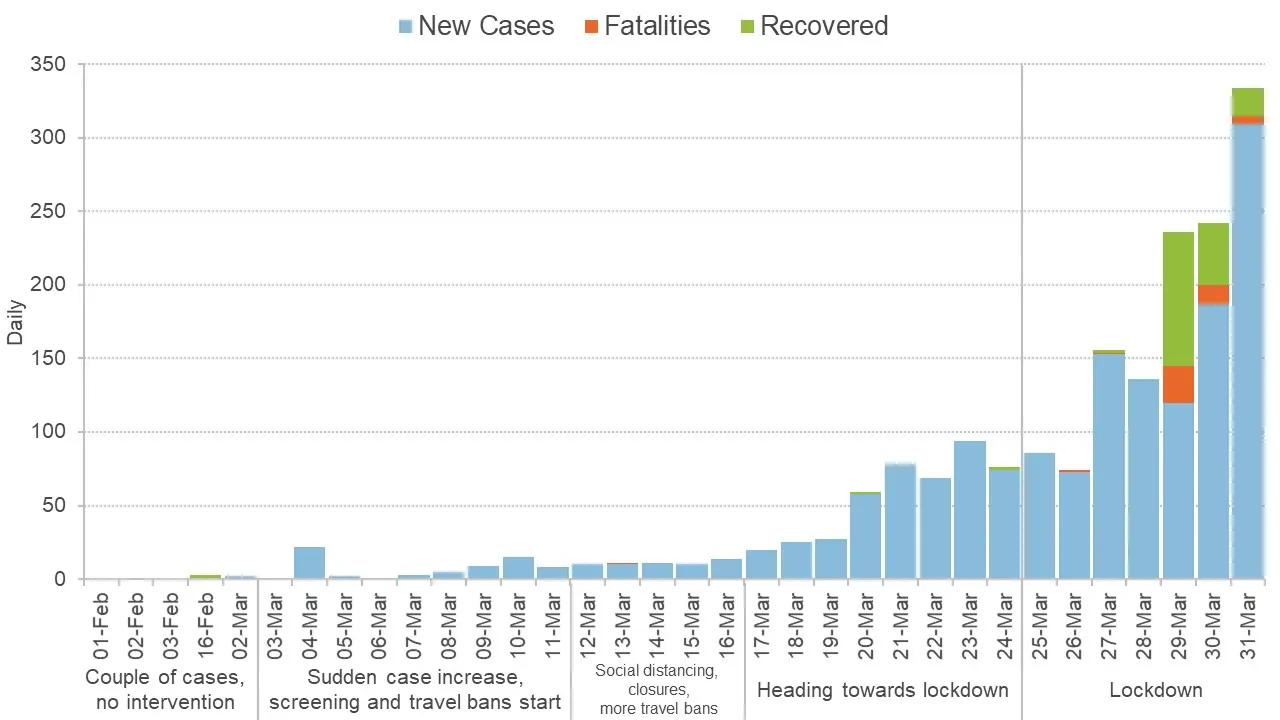
Source: COV-IND Study Group, 2020
Figure 2: The number of new Covid-19 cases, fatalities and recoveries following the lifting of lockdown and other restrictive measures
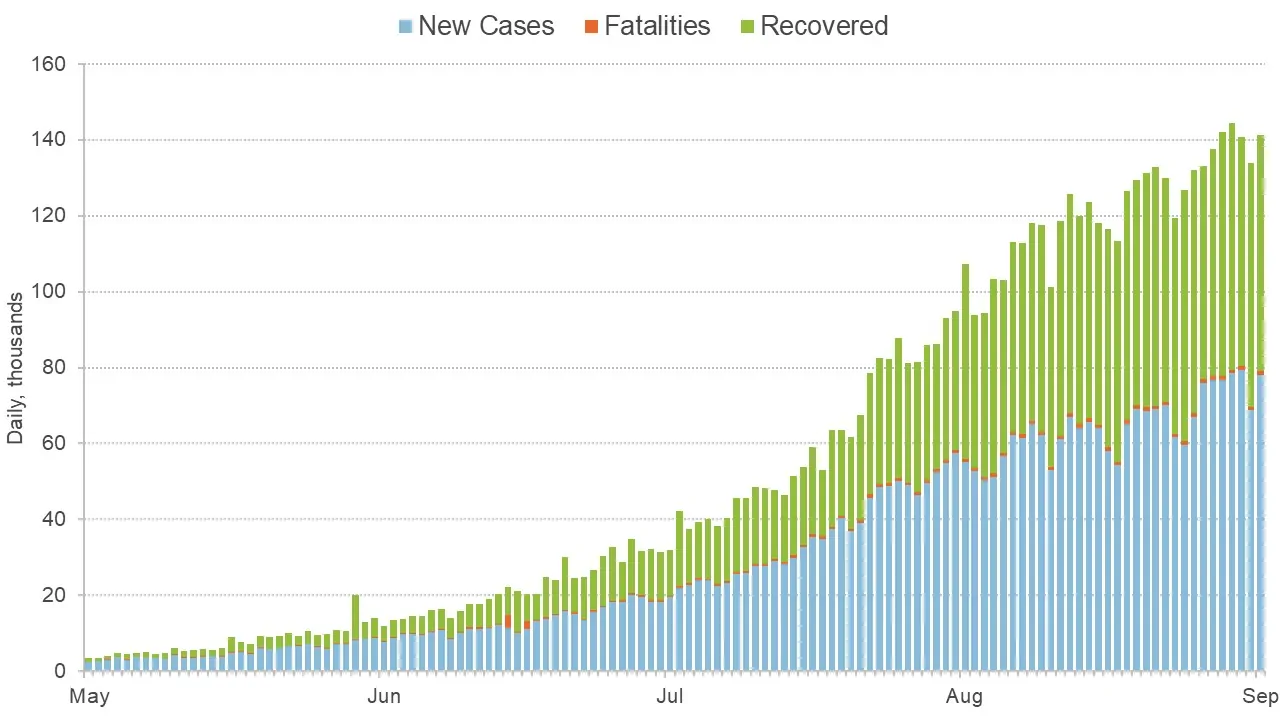
Source: COV-IND Study Group, 2020. Data shows up to 1 September 2020.
Figures 1 and 2 illustrate how restrictive measures in India, including lockdown, the international and domestic travel ban and closing of most businesses except essential services (BBC, 2020), have failed to lead to a decrease in cases when compared with other countries like the UK. The argument that lockdown has resulted in a low CFR is thus refutable.
What is the impact of India’s age structure?
Globally, evidence has also suggested a strong correlation between the Covid-19 mortality rate of a country and the percentage of its population over the age of 65 (Narain, 2020). Countries like France, Italy, Spain and the UK have a very high percentage of population aged over 65 and reported high fatality rates.
Consequently, a widely used explanation to help understand the low CFR in India has been the country’s considerably younger population with a median age of 26.8 (Prasad, 2020). Furthermore, around 27% of the population is estimated to be aged 14 or younger, making it one of the youngest populations in the world.
This view has been supported by evidence from Brazil, which also has a low percentage of the population aged over 65 and a relatively low mortality rate compared with countries like the United States.
On the other hand, data from countries like Germany and Mexico suggest the opposite: Mexico suffered from high mortality despite its low percentage of elderly population; whereas Germany succeeded in minimising Covid-19-related deaths despite the country’s high median age (Narain, 2020). Thus, it is uncertain whether the low CFR can be attributed solely to the younger population in India, although it is likely to have influenced mortality.
Aside from the relatively younger population, virologist Dr Shahid Jameel has also mentioned the constant exposure to other highly prevalent infections like tuberculosis in India as a reason why the population could have a stronger innate immunity (Prasad, 2020). A statement from the health ministry emphasised the significance of traditional medicine in India and its role in boosting the immunity of the population against Covid-19 (Vardhan, 2020). Other reports mention factors like extremely high temperatures and universal BCG vaccinations as contributors to the low CFR (Narain, 2020). There is no scientific evidence to support any of these claims.
Is India missing data?
Most affected countries around the world have inadvertently under-reported deaths during the pandemic. A study by the New York Times analysed mortality data from 12 countries and concluded that at least 40,000 more people would have died during the pandemic than the official death count. This number includes Covid-19 fatalities as well as those who died from other causes.
The same is likely to have happened in India where around 80% of deaths happen at home, including deaths from diseases like malaria and pneumonia (Biswas, 2020). An investigation into the low CFR in India alluded to a host of reasons starting with India’s alarming death reporting rates, as only around 22% of deaths are medically certified (FIT, 2020). The majority of the population are also found in rural areas where most deaths occur at home, thereby delaying registration (see Figure 3).
A report by The Lancet (Chatterjee, 2020) demonstrates the uncertainty that experts feel about India’s Covid-19 mortality data as there is no clarity about how deaths are being registered throughout the country. This is due to the structure of the health system whereby each state is responsible for healthcare, leading to different strategies and guidelines being followed across the country.
Figure 3: Differences in number of cases observed across the Indian states
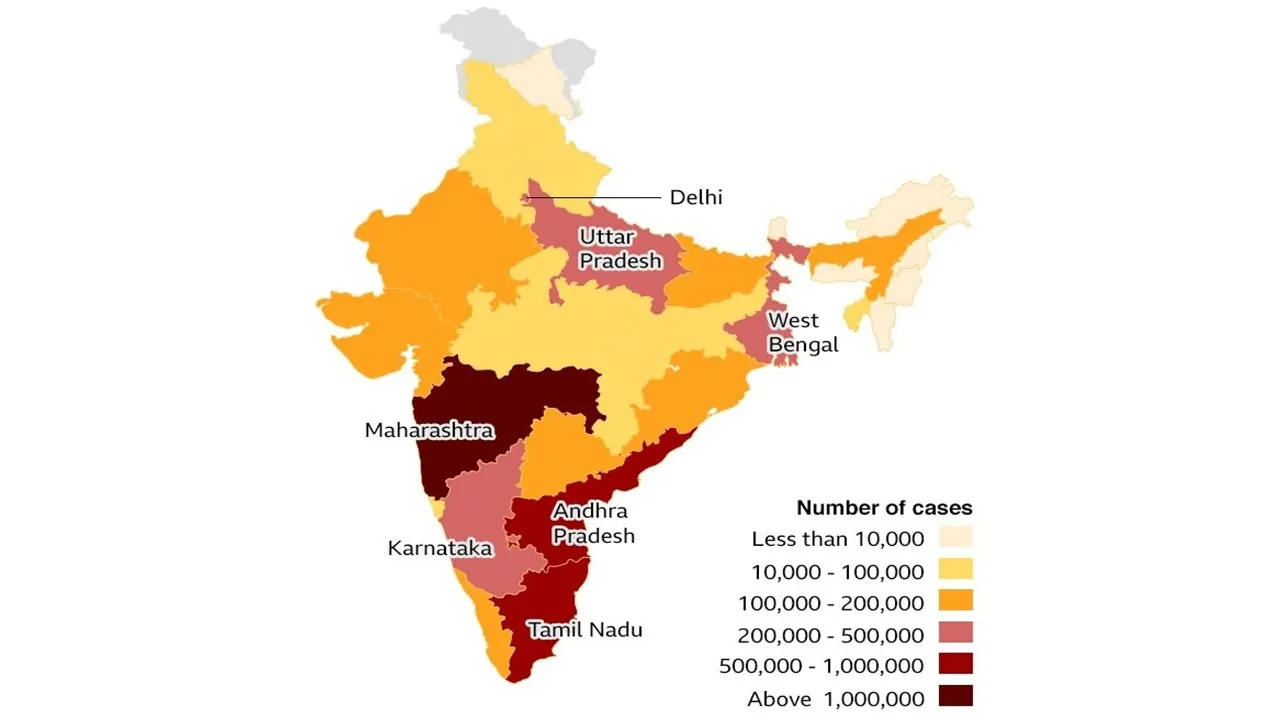
Source: BBC, 2020. Data updated on 16 September 2020.
Researchers have also highlighted the shortcomings in the surveillance mechanisms adopted, as deaths among those who have not been tested are being missed. Case studies from the different states indicate that several patients dying from co-morbidities worsened by Covid-19 are not included in the official death count (Saikia, 2020).
While there is also a commonly held perception that governments tend to be cautious when reporting deaths so as not to scare the public, as Dr Prabhat Jha, who led India’s Million Death Study, says, ‘you can’t hide mass deaths’, and it is unlikely that the actual death count is being hidden intentionally (Biswas, 2020). But it is very likely that the lack of standardisation in testing and data reporting across the country and inefficient surveillance systems have created a gap in the data available.
How is India’s case fatality rate being interpreted?
The CFR is calculated by dividing the number of deaths by the number of confirmed cases. A quantitative analysis of the relevance of infection and Covid-19 deaths finds that there is a time lag occurring between the onset of infection and the date of death (Philip et al, 2020). Consequently, deaths on a particular day divided by the number of cases on the same day may not be an accurate reflection of the true CFR. There are a number of other reasons why the CFR needs to be interpreted cautiously in countries like India.
- First, the widespread lack of testing across the country has resulted in only a fraction of confirmed cases being identified.
- Second, the CFR depicts the number of people dying among the number being diagnosed, and it is distinct from the ‘infection fatality rate’ (IFR), which refers to the number of people dying among the number who are infected. In most countries including India, the number of diagnosed cases is different than the number of those infected.
- Third, using death as an indicator to understand and measure severity requires a Covid-19 death to be certified as such. The only way to do so would be by using an RT-PCR (reverse-transcription polymerase chain reaction) test. But this raises questions about access as a vast proportion of the Indian population suffers from poor access to healthcare and could thus be unable to receive such testing (Pulla, 2020). Unless testing using methods like RT-PCR and antibody tests is increased rapidly, it is likely that the death rate in India will be widely misinterpreted (Sharma, 2020).
- Fourth, the CFR does not take into consideration an exact age-specific distribution of Covid-19 cases and deaths. While countries like India may have a lower CFR as its vastly younger population is resilient to the virus, research (Philip et al, 2020) suggests that the country could actually have a higher age-specific mortality rate while still exhibiting an overall lower mortality.
As cases rise and the recovery rate continues to improve in India, the mystery surrounding the country’s low CFR remains unchanged. It can be concluded that there is no clear explanation for the low deaths despite factors like the lifting of restrictive measures and an overburdened health system.
While the low mortality is good news, it is imperative to understand that it is not necessarily a good sign as there are several complex and unknown factors at play. It is therefore critical for the Indian states and union territories not to become complacent nor to underestimate the severity of the virus. Like most of the world, India still has a long way to go before it can overcome and recover from this pandemic.
Where can I find out more?
Is India missing Covid-19 deaths? A report by Patralekha Chatterjee for The Lancet on India’s Covid-19 mortality data.
Why India’s lockdown has been a spectacular failure: Opinion piece by Indradeep Bhattacharyya on why lockdown in India was a failure.
On India’s ‘low’ Covid-19 case fatality rate: A quantitative analysis of the relevance of age distribution and the time lag between infection and death by Minu Philip, Debraj Ray and S. Subramanian, published at Ideas for India.
Who are experts on this question?
- K. Srinath Reddy, Public Health Foundation of India
- Shahid Jameel, The Wellcome Trust / DBT India Alliance
- Debraj Ray, New York University





































